As for the uptick in cases and hospitalizations without a current increase in deaths:
The spread has largely been from travel hubs with high concentrations of people outward along interstates, state highways, then smaller roads into more rural areas. Larger cities were hit hard first and finally began to see improvement.
Meanwhile, more rural areas took the low numbers of infections as proof it isn't so bad and despite the numbers indicating infections picking up speed in their areas they went ahead with reopening.
A lot of infections flew under the radar for obvious reasons, but the virus was still spreading. It was slowed down by closures and mitigation measures, both mandated and individual choice.
Hospitalizations continued as did deaths. Look at where AL was one month ago compared to now. In just a few weeks AL went from 300 or so deaths and is now closing in on 1,000.
In places like AL you aren't going to see what you saw in NYC except for certain clusters. Montgomery comes to mind as it has reached a "critical mass" there. The population being more spread out is a different situation than high density cities.
We only began seeing hospitalizations from reopening 2-3 weeks ago. I've followed AL most closely and deaths have increased.
Labor Day infections began showing up 2 weeks or so ago. Hospitalizations have been on a general trend upwards. Deaths should lag by 2-3 weeks, so they should be showing up soon.
So some of this is lag. Some of it is the "slow burn" nature of less dense populations. Some areas are fairing better than others while some are obviously doing worse.
The protests should begin showing up soon if not already.
Somewhere between 20 and 25 states are seeing increases in infections, hospitalizations, and/or deaths. This is the reason the numbers are relatively stable. Whereas high density areas were driving the numbers previously less dense areas now are driving the numbers. Because infections are more spread out fewer hospitals are overwhelmed and those that are have a relief valve in the form of other hospitals who can take some of the load off.
How long that is sustainable is anyone's guess.
If you look at the patterns in AL there are peaks and valleys in the data and there appear to be some reporting anomalies. A couple of weeks ago there was a delay in reporting due to some issues with communicating the results. That was ironed out and a dip became a surge. More recently there was a dip. I expect another surge and indeed yesterday's numbers I just checked after writing that show the recent dip and another surge beginning 6/22/20. You can see this trend in new infections and hospitalizations but the state makes tracking deaths much more difficult as there is no quick visual representation on the ADPH site.
As for treatments, it only makes sense that as time has gone on treatment has improved. In the beginning ventilators were likely overutilized based on the previous SARS and MERS outbreak treatments. Harm was likely done but it was the best that was known at the time. That quickly changed, thanks to astute clinicians doing what they do every day. Hydroxychloroquine likely harmed people.
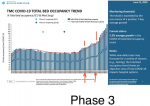
More was learned about the disease in fits and starts. It's widely believed there are two phases - first the infection and then the cytokine storm. Antivirals are more helpful in the first phase. Antibiotics if secondary infection along with tocilizumab, steroids, anticoagulants, diuretics (to remove fluid from the lungs), and a potpourri of other meds for the second phase. High flow oxygen is now preferred throughout treatment over ventilators, which have become a last resort instead of firstline therapy. There is some debate on how much of which anticoagulants to use as COVID-19 cause hypercoagulation (more blood clotting) through an unusual mechanism and current anticoagulants have limited value, but are nonetheless quite valuable.
The evidence is mounting that this is not in any way a "typical" respiratory illness beyond the mode of transmission and that the lungs are majorly affected. Thus virus travels to heart, liver, kidneys, and other organs and directly infects them. It seems to directly infect endothelial tissue (inside lining of blood vessels). Micro and macro clotting is quite common in the lungs and other organs. There are pulmonary emboli, heart attacks, strokes, DVTs, and generally widespread clotting and inflammation from the cytokine storm.
A friend of mine recently died after being on a ventilator plus ECMO and having pulmonary emboli and finally a massive stroke. I haven't been brave enough to ask his wife if it was COVID, but I'm very suspicious as he was previously a healthy man in his mid 50's. The clinical picture I got from her was very similar to what I'd expect, but I have not seen it counted in the county data.
That was a very long and rambling post. Sorry about that.


 www.nbcnews.com
www.nbcnews.com